
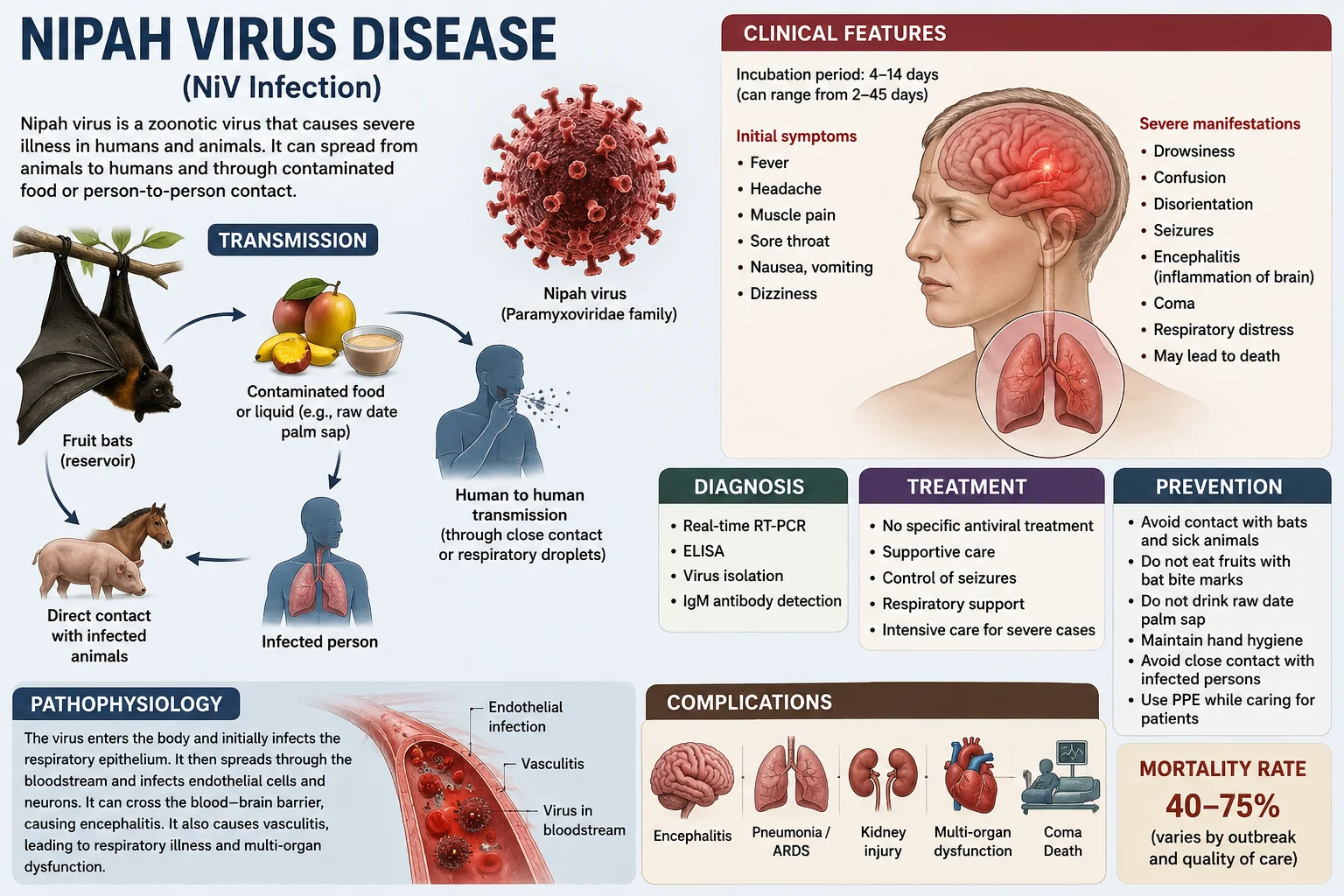
Nipah virus disease is a serious and potentially fatal zoonotic infection caused by the Nipah virus. First identified in 1998 during an outbreak in Malaysia, the disease has since emerged as a significant public health concern in several countries of South and Southeast Asia. Fruit bats of the genus Pteropus, commonly known as flying foxes, are the natural reservoirs of the virus. Humans can become infected through direct contact with infected animals, consumption of contaminated food, or close contact with infected individuals.
Nipah virus infection can range from mild illness to severe respiratory disease and acute encephalitis, an inflammation of the brain that can lead to coma and death. The disease is particularly concerning because of its high mortality rate and its ability to spread from person to person. At present, there is no specific antiviral treatment or licensed vaccine for Nipah virus disease, making prevention and early detection essential. Increasing public awareness about its transmission, symptoms, and preventive measures is crucial for reducing the risk of outbreaks and protecting community health.
The name Nipah was derived from Kampung Sungai Nipah, a village in Malaysia where the virus was first identified during the 1998–1999 outbreak.
Therefore:
NIPAH = No full form
Nipah = Name of the village where the virus was first discovered.
Prevalence of Nipah Virus Disease in West Bengal
West Bengal has experienced three documented Nipah virus outbreaks. The first occurred in Siliguri in 2001, involving approximately 66 cases with a high fatality rate. A second outbreak occurred in Nadia district in 2007, resulting in 5 confirmed deaths. More recently, WHO reported another outbreak in North 24 Parganas (Barasat) in 2026, involving two laboratory-confirmed cases among healthcare workers. These events indicate that Nipah virus remains rare in West Bengal but has caused sporadic outbreaks with significant mortality.
Study links:
Siliguri outbreak (2001):
Nipah Virus-associated Encephalitis Outbreak Siliguri, India Study
https://pmc.ncbi.nlm.nih.gov/articles/PMC3373078/?utm_source=chatgpt.com
Nadia outbreak (2007):
Genomic Characterization of Nipah Virus, West Bengal, India Study
https://pmc.ncbi.nlm.nih.gov/articles/PMC3321761/?utm_source=chatgpt.com
West Bengal outbreak (2026 WHO report):
WHO Nipah Virus Disease India West Bengal Outbreak Report
Prevalence of Nipah Virus Disease in India
India has reported periodic Nipah outbreaks since 2001. Most outbreaks have occurred in West Bengal and, since 2018, in the state of Kerala. Kerala has become India's principal hotspot, experiencing multiple outbreaks and isolated cases between 2018 and 2026. Although the total number of cases remains low compared with many infectious diseases, Nipah is considered a major public health concern because of its high case-fatality rate (40–75%).
Study links:
Kerala outbreak study (2018):
Clinico Epidemiological Study of Nipah Virus Infection in Kerala, India, 2018
https://pmc.ncbi.nlm.nih.gov/articles/PMC7045760/?utm_source=chatgpt.com
https://www.who.int/news-room/fact-sheets/detail/nipah-virus?utm_source=chatgpt.com
WHO Nipah Virus Fact Sheet:
Recent Kerala outbreak analysis:
Encephalitis Predominant Nipah Virus Outbreaks in Kerala, India, During 2024
Global Prevalence of Nipah Virus Disease
Globally, Nipah virus disease is considered a rare but emerging zoonotic infection. Since its first identification in Malaysia in 1998, human cases have been reported mainly in Malaysia, Singapore, Bangladesh, India, and the Philippines. Bangladesh and India continue to report periodic outbreaks, while Malaysia and Singapore have not reported new outbreaks since 1999. The disease remains geographically limited but is recognized by the WHO as a priority pathogen because of its epidemic potential and high mortality.
Study links:
WHO Global Nipah Virus Overview:
WHO Nipah Virus Fact Sheet:
Short Summary
West Bengal: Three documented outbreaks (2001, 2007, 2026).
India: Sporadic outbreaks, mainly in West Bengal and Kerala.
World: Rare disease, reported mainly in South and Southeast Asia, but of global concern because of its high fatality rate and outbreak potential.
Causes of Nipah Virus Disease:
Nipah virus disease is caused by infection with the Nipah virus, a highly infectious member of the genus Henipavirus. The virus can spread to humans through several routes:
1. Contact with infected fruit bats – Fruit bats of the genus Pteropus are the natural reservoir of the virus. Their saliva, urine, or droppings can contaminate food and water.
2. Consumption of contaminated food – Eating fruits or drinking raw date palm sap contaminated by infected bats can transmit the virus.
3. Contact with infected animals – Pigs and some other animals can become infected and pass the virus to humans.
4. Human-to-human transmission – Close contact with an infected person's respiratory secretions, saliva, urine, blood, or other body fluids can spread the disease.
5. Hospital-associated transmission – Healthcare workers and caregivers may become infected while caring for Nipah patients without adequate infection-control measures.
Clinical Manifestations of Nipah Virus Disease
The clinical manifestations of Nipah virus disease range from asymptomatic infection to severe respiratory illness and fatal encephalitis.
1. General (Prodromal) Manifestations
Fever, Headache, Malaise and fatigue, Myalgia (muscle pain), Sore throat, Nausea, and vomiting
2. Respiratory Manifestations
Cough, Shortness of breath (dyspnea), Tachypnea (rapid breathing), Pneumonia, Acute respiratory distress syndrome (ARDS)
3. Neurological Manifestations
Dizziness, Drowsiness, Confusion, Disorientation, Altered level of consciousness, Seizures, Encephalitis (brain inflammation), Coma
4. Autonomic and Systemic Manifestations
Tachycardia (rapid heart rate), Blood pressure instability, and multi-organ dysfunction in severe cases
5. Long-Term Neurological Sequelae
Among survivors, some may develop: Persistent fatigue, Personality and behavioral changes, Memory impairment, Difficulty concentrating, Recurrent seizures, and residual neurological deficits
Key Clinical Feature
The hallmark clinical manifestation of Nipah virus infection is acute encephalitis, often accompanied by respiratory involvement, with rapid progression and a high risk of mortality.
Pathophysiology of Nipah Virus Disease
Nipah virus disease is caused by the Nipah virus (NiV), a zoonotic virus in the genus Henipavirus. The disease develops through a series of steps that involve viral entry, spread through the body, blood vessel damage, and inflammation of the brain and lungs.
1. Viral Entry
The virus enters the body through the respiratory tract or gastrointestinal tract.
Infection occurs after contact with infected bats, pigs, contaminated food, or infected humans.
2. Initial Replication
After entry, the virus replicates in the epithelial cells of the respiratory tract.
From the local site of infection, it enters the bloodstream, causing viremia.
3. Systemic Spread
The virus spreads to multiple organs, particularly the lungs, brain, spleen, kidneys, and heart.
It has a strong affinity for endothelial cells, which line the blood vessels.
4. Vascular Damage
Infection of endothelial cells leads to vasculitis (inflammation of blood vessels).
The damaged vessels become leaky, causing edema, hemorrhage, and impaired blood flow.
This vascular injury is a major contributor to organ dysfunction.
5. Central Nervous System Involvement
The virus crosses the blood–brain barrier through infected endothelial cells and immune cells.
It infects neurons and supporting brain cells, resulting in encephalitis.
Inflammation and swelling of the brain cause symptoms such as headache, confusion, seizures, coma, and neurological deficits.
6. Respiratory Involvement
The virus can directly infect lung tissue, leading to pneumonia and acute respiratory distress syndrome (ARDS).
Severe respiratory failure may occur, especially in advanced disease.
7. Severe Disease and Outcome
The combination of brain inflammation, vascular damage, and respiratory failure can lead to multi-organ dysfunction.
Without prompt supportive care, severe cases may progress rapidly to coma and death.
In summary
Nipah virus enters through the respiratory or digestive tract, spreads through the bloodstream, damages blood vessels, and invades the brain and lungs. The resulting vasculitis, encephalitis, and respiratory injury are responsible for the severe clinical manifestations and high mortality associated with the disease.
Prevention and Control of Nipah Virus Disease in the Community
Preventing and controlling Nipah virus disease requires reducing exposure to infected animals, contaminated food, and infected individuals, along with strengthening public health measures.
1. Avoid Contact with Fruit Bats and Sick Animals
Do not handle bats or animals that appear sick.
Avoid areas where bats commonly roost.
Report unusual illness or deaths among animals to authorities.
2. Consume Safe Food and Water
Avoid eating fruits that have been partially eaten or contaminated by bats.
Wash fruits thoroughly before consumption.
Avoid drinking raw date palm sap or other foods that may be contaminated by bat saliva or urine.
Drink safe, clean water.
3. Practice Good Personal Hygiene
Wash hands regularly with soap and water.
Use alcohol-based hand sanitizers when soap and water are unavailable.
Cover the mouth and nose while coughing or sneezing.
4. Prevent Person-to-Person Transmission
Avoid close contact with infected individuals.
Do not share personal items such as utensils, towels, or bedding with patients.
Follow isolation measures for suspected or confirmed cases.
5. Use Protective Equipment
Caregivers and healthcare workers should wear masks, gloves, gowns, and eye protection when caring for patients.
Follow proper infection prevention and control practices.
6. Strengthen Surveillance and Early Detection
Report suspected cases promptly to health authorities.
Conduct contact tracing and monitor exposed individuals.
Establish rapid laboratory diagnosis and outbreak response systems.
7. Community Awareness and Health Education
Educate the public about transmission, symptoms, and prevention of Nipah virus disease.
Promote awareness through schools, community meetings, and mass media.
Encourage early medical consultation for fever, respiratory symptoms, or neurological signs.
8. Safe Management of Patients and Deceased Persons
Ensure proper infection-control measures during patient care.
Follow recommended guidelines for the safe handling and burial of deceased patients.
Conclusion
Community prevention and control of Nipah virus disease depend on avoiding exposure to bats and contaminated foods, maintaining good hygiene, preventing person-to-person transmission, ensuring early detection of cases, and promoting public awareness. These measures are essential to prevent outbreaks and protect public health.
Outline of Treatment Measures for Nipah Virus Disease
Currently, there is no specific antiviral drug or licensed vaccine approved for Nipah virus disease. Treatment is mainly supportive and symptomatic.
1. Hospitalization and Isolation
Admit suspected or confirmed cases to a healthcare facility.
Isolate patients to prevent person-to-person transmission.
Implement strict infection prevention and control measures.
2. Supportive Care
Maintain adequate hydration and electrolyte balance.
Provide nutritional support.
Monitor vital signs and organ function closely.
3. Management of Fever and Pain
Administer antipyretics (e.g., paracetamol) to reduce fever.
Provide analgesics for headache and body aches.
4. Respiratory Support
Provide supplemental oxygen for breathing difficulties.
Use mechanical ventilation when respiratory failure develops.
Manage acute respiratory distress syndrome (ARDS) in intensive care settings.
5. Neurological Management
Monitor for signs of encephalitis.
Control seizures with appropriate anticonvulsant medications.
Manage increased intracranial pressure and cerebral edema when present.
In severe Nipah virus encephalitis, doctors reduce brain swelling (cerebral edema) and intracranial pressure by:
Elevating the head of the bed (about 30°) improves venous drainage from the brain.
Administering osmotic agents such as mannitol or hypertonic saline to draw excess fluid out of brain tissue.
Ensuring adequate oxygenation and ventilation.
Monitoring and controlling fever, seizures, and blood pressure.
Providing intensive care support and close neurological monitoring.
These measures help prevent further brain damage and reduce the risk of coma and death.
6. Intensive Care Management
Continuous monitoring of critically ill patients.
Support cardiovascular and respiratory functions.
Manage complications such as shock and multi-organ dysfunction.
7. Experimental Therapies
Some antiviral agents and monoclonal antibodies have been investigated in research settings.
Their use remains limited and is generally guided by national health authorities and clinical protocols.
8. Infection Prevention During Care
Healthcare workers should use personal protective equipment (PPE).
Follow strict hand hygiene and isolation precautions.
Conclusion
The treatment of Nipah virus disease is primarily based on early diagnosis, isolation, supportive care, respiratory support, neurological management, and intensive care when required. Prompt medical attention can improve outcomes and help prevent the spread of infection.