
Education plays a vital role in the successful treatment and long-term management of gout. When people understand the causes, symptoms, treatment options, and lifestyle changes associated with gout, they are better equipped to manage the condition effectively. Learning about the importance of taking prescribed medications, following a healthy diet, staying physically active, maintaining a healthy body weight, and avoiding known triggers can help control uric acid levels and reduce the frequency of gout attacks. Educating people also promotes early recognition of symptoms, timely medical care, and better adherence to treatment, ultimately preventing future flare-ups, joint damage, kidney complications, and improving overall quality of life.
Treatment of Gout
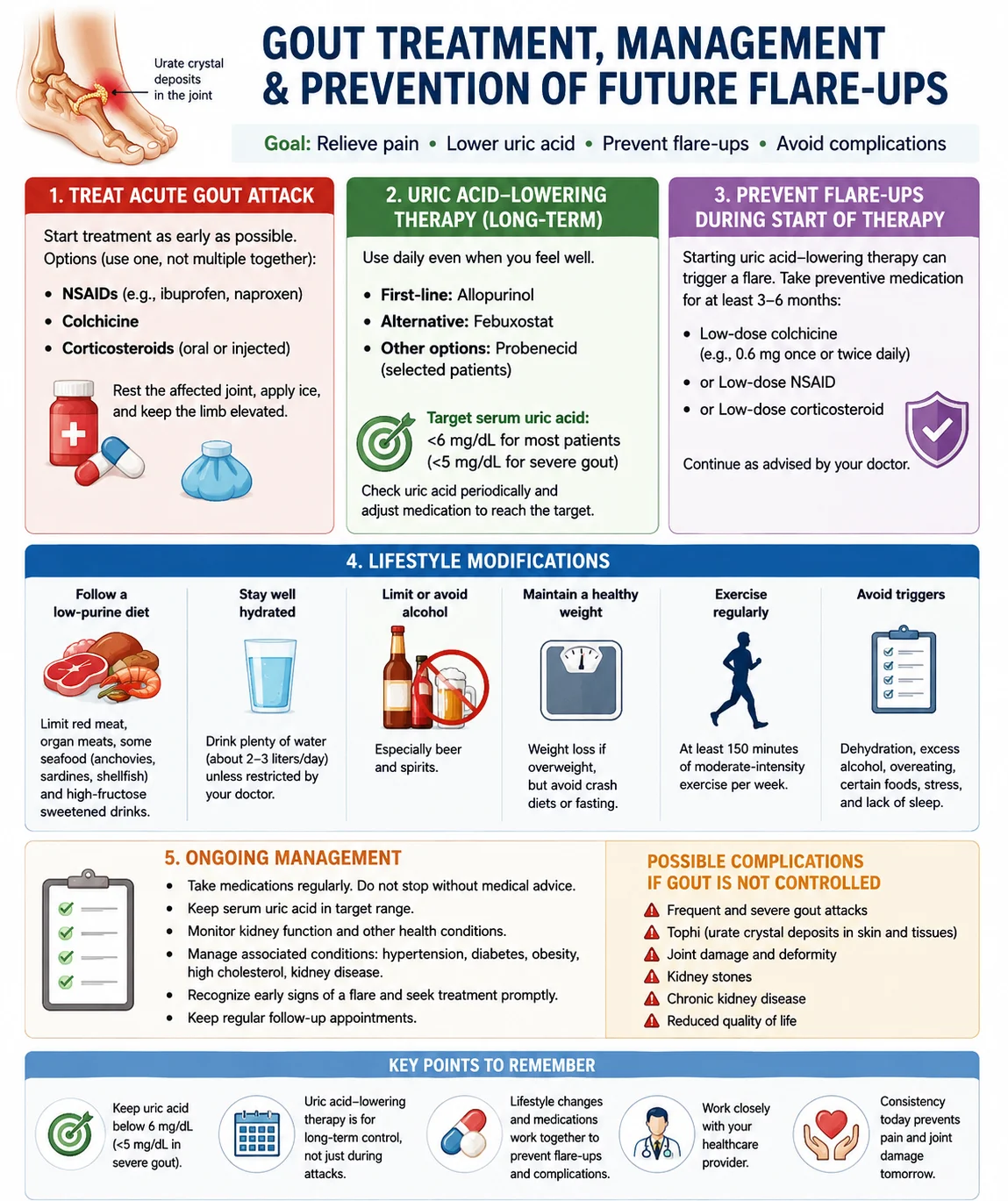
1. Treat acute gout attacks
i). Nonsteroidal anti-inflammatory drugs (NSAIDs-e.g., ibuprofen, naproxen) Nonsteroidal anti-inflammatory drugs (e.g., Ibuprofen and Naproxen) act by blocking the #cyclooxygenase (COX-1 and COX-2) enzymes, which reduces the production of prostaglandins—chemicals responsible for pain, inflammation, and swelling.
#Cyclooxygenase (COX-1 and COX-2) enzymes are enzymes that convert arachidonic acid into prostaglandins. Prostaglandins are chemical messengers that dilate blood vessels, increase blood flow and blood vessel permeability, and thus stimulate pain receptors, leading to pain, inflammation, swelling, and fever. NSAIDs work by blocking COX enzymes, thereby reduce prostaglandin production and become responsible for pain, inflammation, and swelling.
https://www.ncbi.nlm.nih.gov/sites/books/NBK549795/?utm_source=chatgpt.com
ii). Colchicine
It works by reducing the inflammatory response to #monosodium urate (MSU) crystals in the joints.
Monosodium urate (MSU) crystals are needle-shaped crystals formed from excess uric acid that deposit in joints and cause gout.
How does Colchicine act?
Neutrophils are the most common type of white blood cells and are the body's first line of defense against infection and injury. When monosodium urate (MSU) crystals deposit in a joint, neutrophils move to the affected joint, engulf (try to digest) the urate crystals, release inflammatory chemicals, which cause pain, swelling, redness, warmth, and tenderness. But colchicine inhibits neutrophil (white blood cell) to migrate to the affected joint and thereby no inflammatory responses occur, so pain is relieved. Colchicine does not lower blood uric acid levels or dissolve urate crystals. It only reduces inflammation caused by the crystals.
https://www.ncbi.nlm.nih.gov/books/NBK431102/?utm_source=chatgpt.com
Reduces the release of inflammatory chemicals (cytokines).
Monosodium urate crystals in the joint activate immune cells.
>These immune cells release cytokines (chemical messengers), particularly #IL-1β.
#IL-1β (Interleukin-1 beta) is a pro-inflammatory cytokine (chemical messenger) that triggers pain, swelling, redness, and inflammation during a gout attack.
>IL-1β attracts more neutrophils and amplifies inflammation, causing severe pain, swelling, redness, and warmth.
>Colchicine blocks neutrophil activation and migration, which reduces the release of IL-1β and other inflammatory cytokines.
>As a result, the inflammatory response decreases and the symptoms of a gout attack improve.
Main reference:
StatPearls – Colchicine
https://www.ncbi.nlm.nih.gov/books/NBK431102/?utm_source=chatgpt.com
Important: Colchicine does not lower blood uric acid levels or dissolve urate crystals. It only reduces inflammation caused by the crystals.
iii). Corticosteroids (oral or injected)
>Reduce the production of inflammatory cytokines (such as IL-1β and #TNF-α).
#TNF-α (Tumor Necrosis Factor-alpha) is a pro-inflammatory cytokine (chemical messenger) that promotes inflammation by attracting immune cells and increasing pain, swelling, redness, and tissue damage.
>Decrease the activity of white blood cells, including neutrophils.
>Reduce blood vessel permeability, decreasing fluid leakage into the joint.
>Relieve pain, swelling, redness, and stiffness during an acute gout attack.
Important: Corticosteroids do not lower blood uric acid levels. They only reduce the inflammation caused by uric acid crystals.
Main research/guideline link
2020 American College of Rheumatology Guideline for the Management of Gout
https://rheumatology.org/gout-guideline?utm_source=chatgpt.com
2. Lower blood uric acid levels (long-term treatment)
i). Allopurinol (first-line treatment)
Allopurinol is the first-line medicine for the long-term treatment of gout. It lowers blood uric acid levels by blocking the enzyme #Xanthine oxidase, which converts purines into uric acid.
#Xanthine oxidase is an enzyme that converts purines into uric acid in the body.
How does Allopurinol act?
>Blocks the xanthine oxidase enzyme.
>Reduces the production of uric acid.
>Prevents the formation of new monosodium urate crystals.
>Allows existing urate crystals to gradually dissolve, reducing gout attacks over time.
Important: Allopurinol does not relieve pain during an acute gout attack. It is used long-term to prevent future attacks by keeping blood uric acid levels low.
Main research/guideline link:
2020 American College of Rheumatology Guideline for the Management of Gout
https://rheumatology.org/gout-guideline?utm_source=chatgpt.com
ii). Febuxostat
Febuxostat treats gout by lowering blood uric acid levels. Like allopurinol, it blocks the enzyme Xanthine oxidase, which converts purines into uric acid.
So, Febuxostat does not relieve pain during an acute gout attack. It is used for long-term control of blood uric acid levels and prevention of recurrent gout.
Main research/guideline link:
2020 American College of Rheumatology Guideline for the Management of Gout
iii). Probenecid (in selected patients)
Probenecid treats gout by helping the kidneys remove more uric acid from the body.
How does Probenecid act?
>Blocks the reabsorption of uric acid in the kidney tubules.
Normally, the kidneys filter uric acid from the blood, but some of it is taken back (reabsorbed) into the bloodstream through the kidney tubules. Probenecid blocks this reabsorption, so more uric acid stays in the urine and is removed from the body.
>Increases the excretion of uric acid in urine.
>Lowers blood uric acid levels.
>Prevents the formation of new urate crystals and helps existing crystals gradually dissolve, reducing future gout attacks.
Important: Probenecid does not relieve pain during an acute gout attack. It is used for long-term prevention of gout in #selected patients who can adequately excrete uric acid through their kidneys.
#Selected patients: The patients with gout whose kidneys still work well but do not remove enough uric acid naturally. It helps the kidneys excrete more uric acid into the urine. It is often used when allopurinol or febuxostat cannot be used or are not effective. It is usually not recommended for people with significant kidney disease or a history of uric acid kidney stones.allopurinol or febuxostat cannot be used
Allopurinol or febuxostat may not be used if the patient has:
Severe allergy or serious adverse reactions to the drug.
Certain heart diseases (especially for febuxostat).
Conditions where the risks outweigh the benefits, as determined by a healthcare provider.
Main research/guideline link:
2020 American College of Rheumatology Guideline for the Management of Gout
https://rheumatology.org/gout-guideline?utm_source=chatgpt.com
3. Lifestyle modifications
Follow a low-purine diet.
Drink plenty of water.
Maintain a healthy body weight.
Limit alcohol and sugary beverages.
Exercise regularly.
4. Manage underlying medical conditions
Control obesity, diabetes, hypertension, and kidney disease.
5. Regular monitoring and follow-up
i). Check serum uric acid levels periodically.
For people with gout or taking urate-lowering therapy, current guidelines recommend:
How often should serum uric acid be checked?
Every 2–5 weeks after starting or changing uric acid-lowering medication until the target uric acid level is reached.
Every 6–12 months once the target level is stable and gout is well controlled.
What uric acid level should be maintained?
Target for most people with gout: <6 mg/dL (<360 µmol/L)
Target for severe gout (e.g., tophi or frequent attacks): <5 mg/dL (<300 µmol/L)
Keeping uric acid below these targets helps prevent the formation of new monosodium urate crystals and allows existing crystals to gradually dissolve, reducing future gout attacks.
Main research/guideline link:
The target of <6 mg/dL (360 µmol/L) is recommended for most patients with gout by the 2020 American College of Rheumatology Guideline for the Management of Gout.
This guideline recommends treating acute inflammation promptly and using urate-lowering therapy, especially allopurinol, for long-term prevention of recurrent gout attacks and complications.
Possible Complications of Untreated or Poorly Managed Gout
i). Recurrent gout attacks – Frequent episodes of severe joint pain and inflammation.
ii). Tophi formation – Hard deposits of urate crystals under the skin, commonly around the fingers, toes, elbows, and ears.
iii). Permanent joint damage and deformity – Chronic inflammation and crystal deposits can destroy cartilage and bone, leading to reduced joint function.
iv). Uric acid kidney stones – Excess uric acid can form stones in the urinary tract, causing severe pain and urinary obstruction.
v). Chronic kidney disease – Long-term urate crystal deposition and recurrent kidney stones may impair kidney function.
vi). Reduced mobility and disability – Repeated joint damage can make walking and daily activities difficult.
vii). Increased risk of cardiovascular disease – Gout is associated with a higher risk of heart disease and stroke, especially when accompanied by hypertension, obesity, or diabetes.
viii). Reduced quality of life – Chronic pain, disability, and frequent flare-ups can affect work, sleep, and emotional well-being.
Main research/guideline link
2020 American College of Rheumatology Guideline for the Management of Gout
This guideline emphasizes that maintaining serum uric acid below 6 mg/dL and adhering to long-term treatment can prevent these complications.
Goals of management
Prevent recurrent gout attacks.
Prevent Tophi (urate crystal deposits under the skin).
Prevent joint damage and deformity.
Prevent uric acid kidney stones and chronic kidney disease.
Improve quality of life.
Management of Patients with Gout
Take uric acid-lowering medications as prescribed (e.g., allopurinol or febuxostat).
Treat acute gout attacks promptly with appropriate anti-inflammatory medications.
Maintain serum uric acid below 6 mg/dL (below 5 mg/dL in severe gout).
Follow a balanced low-purine diet and avoid high-purine foods.
Drink plenty of water (about 2–3 L/day unless medically restricted).
Maintain a healthy body weight and avoid crash diets.
Limit or avoid alcohol and avoid sugar-sweetened beverages.
Exercise regularly (at least 150 minutes of moderate-intensity activity per week).
Manage associated conditions such as obesity, diabetes, hypertension, and kidney disease.
Take medications regularly and do not stop them without medical advice.
Monitor serum uric acid and kidney function regularly and adjust treatment as needed.
Recognize early signs of a flare-up and seek treatment promptly.
Avoid known triggers, such as dehydration, excessive alcohol, overeating purine-rich foods, and prolonged fasting.
Attend regular follow-up visits with a healthcare provider.
Learn about gout and its long-term management to improve treatment adherence and prevent complications.
Main guideline:
2020 American College of Rheumatology Guideline for the Management of Gout